The emergency visibility crisis nobody built a solution for — until now.
Fifty years of academic research, policy white papers, conference panels, and government task forces have documented America's ambulance desert crisis with extraordinary precision. They have mapped it, measured it, modeled it, and published it in every journal that would take it. The number of people living in ambulance deserts has not decreased by a single person. An engineer in Scottsdale, Arizona decided that building a solution was more productive than describing the problem.
The Glomensio Firefly in SOS mode: visible from over 1,000 feet. Built by an engineer. Not recommended by a committee.
Source: Maine Rural Health Research Center, Ambulance Deserts: Geographic Disparities in the Provision of Ambulance Services, May 2023. Analysis of 41 states. Nine states lacked data — true figures are likely higher.
“God may be omnipresent, but EMS isn't.”
— Gaurav Batta, Founder, Glomensio
An ambulance desert is any location where residents live more than 25 minutes from the nearest ambulance station. The term was formalized in a landmark 2023 study by the Maine Rural Health Research Center, led by Yvonne Jonk, PhD and her colleagues. Their analysis of 41 states found that 4.5 million Americans live in these deserts — with 2.3 million of them in rural counties.
The geography is predictable: Appalachia, the rural Mountain West, the coastal fringes of Maine and Oregon, and vast stretches of the Great Plains where eight states have fewer than three ambulances covering every 1,000 square miles. But the crisis is not limited to remote terrain. Ambulance deserts exist in suburban counties, in communities that lost their local hospital, and in towns where the last volunteer EMS provider aged out and nobody replaced them.
In Pickens County, Alabama, a single ambulance station serves nearly 20,000 residents across 900 square miles. In May 2023, Grena Prude, age 55, died of cardiac arrest at Carrollton City Hall — less than half a mile from that station — because both available ambulances were transporting patients to hospitals 30 and 45 minutes away. There was no one left to respond.
Alabama ranks second nationally with 315,000 residents living in ambulance deserts. The county's hospital closed in March 2020, eliminating $250,000 in annual ambulance service revenue overnight. Residents drove 2.5 hours to the state capitol to protest lawmakers' refusal to fund the $8 million hospital reopening. The lawmakers did not fund it.
“Ambulance services were never intended to take the place of emergency departments.”
— Vicky McCrory, Supervisor, Pickens County Ambulance Service (CBS News)
Unlike police and fire departments, EMS is not classified as an essential service in most states. This single policy failure cascades into every aspect of the crisis:
“Of all the poorly designed aspects of our health care system, [EMS] tops.”
— Alan Morgan, CEO, National Rural Health Association (CBS News)
I want to be clear about something: the researchers who have documented America's ambulance desert crisis have done rigorous, important work. Yvonne Jonk's chartbook at the Maine Rural Health Research Center is the definitive geographic analysis. John Gale's EMS performance measures give rural agencies a framework to evaluate themselves. Nick Nudell's 20 years of paramedicine inform every policy discussion on the subject. The Vox documentary below brought the crisis to a mainstream audience. PBS, CBS, and Governing magazine have all covered it with depth and seriousness.
None of it has produced a single product that reduces emergency response time.
This is not a criticism of their intent. It is an observation about the limits of their approach. The academic and policy ecosystem has a structural bias toward more research, more funding proposals, and more committee recommendations. The output is consistently the same: a paper that describes the problem with greater precision, a policy brief that recommends someone else solve it, and a funding request that asks taxpayers to finance the recommendation.
Gale, Coburn, Pearson et al. publish Developing Program Performance Measures for Rural EMS. Expert panel identifies 17 performance measures. Zero are products. Zero are deployed devices. All 17 are measurement frameworks.
Jonk et al. publish Ambulance Deserts: Geographic Disparities in the Provision of Ambulance Services. The crisis is mapped. 4.5 million people identified. The paper recommends “strategic repositioning” of existing ambulances — a proposal that would require every ambulance agency in 41 states to cooperate with a centralized relocation plan that no government entity has the authority to execute.
Jonk et al. publish Consensus Panel on Start-Up and Annual Costs for Rural Ambulance Agencies. Finding: it costs $1.04 million per year to run a minimum-access ambulance station in a low-volume area. The paper establishes cost benchmarks. It does not identify how to fund them, except to note that someone should.
Minnesota allocates $30 million for rural EMS. Maine backs a $31 million sustainability plan. Colorado launches a task force. Alabama's legislature declines to fund an $8 million hospital reopening. Across the country: a patchwork of incremental state-level actions, none coordinated, none sufficient.
Gaurav Batta drops out of a graduate program at Arizona State University to build the Glomensio Firefly — an illuminated house number with an emergency SOS beacon visible from 1,000+ feet. It wins a CES Innovation Award. It earns Batta an EB1A “Einstein Visa” for extraordinary ability in smart home innovation and public safety technology. It ships to customers. It works.
I did not need anyone's permission to solve this problem. I did, however, reach out to some of the people in this space — including the Vox team and Dr. Jonk — to explore collaboration. I never heard back. So I built the table while they continued talking about how hard the floor is. That is the difference between an engineer and an analyst. An analyst describes the world. An engineer changes it.
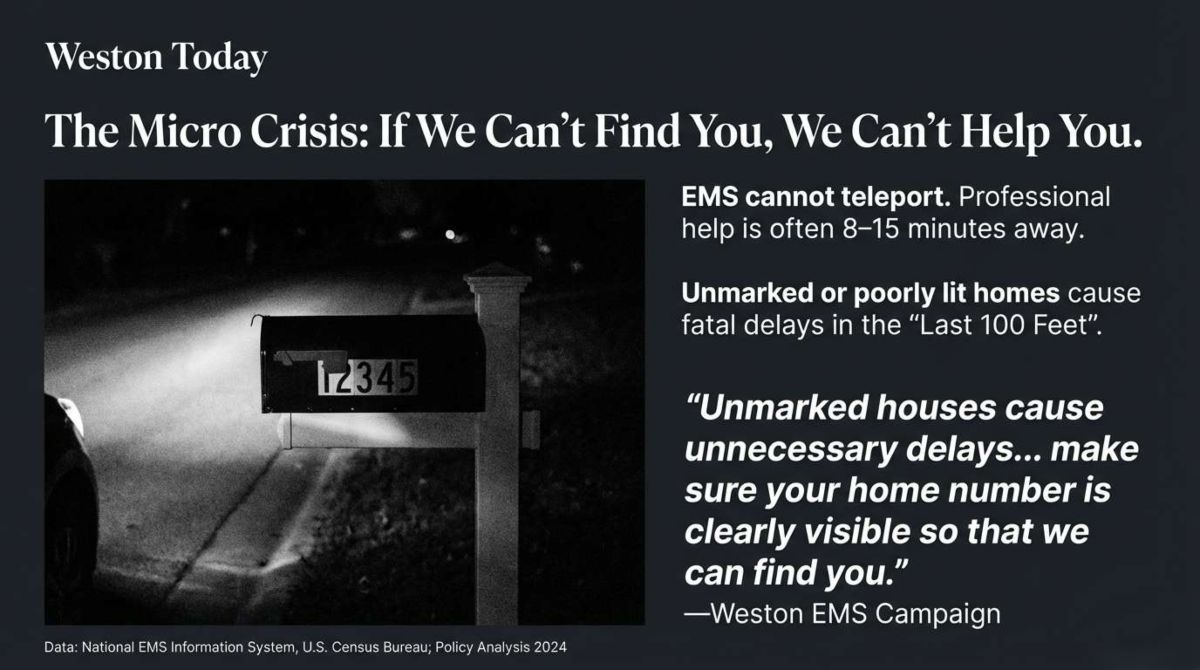
Every ambulance desert study measures the time from station to scene. Not one measures what happens when the ambulance arrives on your street and cannot find your house.
Fire departments across the country have been begging homeowners to fix this for decades. Auburn, Indiana's Fire Chief Michael VanZile put it simply: “Firefighters, EMS responders and police officers cannot provide emergency services to you or your family if we cannot find your house.” The San Bernardino County Fire Department's Tracey Martinez: “Those extra minutes spent trying to locate a property can mean the difference between life and death.” Weston, Connecticut's EMS: “If we can't find you, we can't help you.”
The Houston Herald published Assistant Fire Chief Michael Drozdo's plea that 911 address signs save seconds and lives — noting that in rural areas, “it is very difficult to see decorative or old numbering on a mailbox. Sometimes it is completely non-existent.”
73% of out-of-hospital cardiac arrests occur in homes. Only 40% of those victims receive any help before professionals arrive. That leaves an estimated 190,000 Americans each year in a silent emergency — often within yards of neighbors who have no idea it's happening. In an ambulance desert with 25+ minute response times, a hard-to-find house doesn't add frustration. It adds death.
The research community has not once measured this compounding effect. They measure distance to station. They do not measure findability at destination. That gap — the last 100 feet of the last mile — is where people die while the ambulance is already on their street.
This is the gap I built the Firefly to close.

I did not set out to solve the ambulance desert crisis. I set out to solve a simpler question: why is there no house number that tells a first responder “this is the house” during a medical emergency?
I am a mechanical engineer with an electromechanical specialization. I came to the United States from India in 2012 to study at Arizona State University. I spent years in industry where prototypes ship, not where papers publish. When I left my graduate program in 2021 to build Glomensio, it was because I believed that a product that works is worth more than a thesis that explains why something should work. Read the full story →
The Glomensio Firefly is an illuminated house number with four operating modes, including an automatic emergency SOS beacon that strobes red and blue — visible from over 1,000 feet. When someone in your home calls 911, the Firefly activates. First responders see it from the end of the block. They do not slow down to squint at faded brass numbers. They do not pass your house twice. They arrive.
SOS beacon visible from over 1,000 feet in emergency mode. First responders see your house before they see your street sign.
Linked to your emergency call. No buttons to press, no apps to open during a crisis. The system activates when you need it most.
No batteries to die. No solar panels to degrade. No Wi-Fi dependency during power outages. Hardwired to your home's electrical system with backup power.
Firefly Gen 3 won the CES Innovation Award 2026 — the premier consumer electronics award, judged by an independent panel of industry experts.
“Much like the seatbelt, Firefly doesn't directly treat patients — but it creates the conditions that allow others to do so. Seatbelts were not invented by hospitals, yet they are one of the most consequential public health interventions in history. In the same way, Firefly offers the rare kind of engineering that enables survival without ever stepping into the clinical setting itself.”
— Dr. Thomas Burman, DNP, CRNA, Nurse Anesthesiologist
The Firefly works right now, on your house, regardless of whether your state classifies EMS as essential, whether your county has adequate funding, or whether any researcher has gotten around to studying your particular ambulance desert. It created an entirely new product category — a patented, smart, emergency-triggered address number with international applications pending.
I did not need a grant, a committee, a peer review panel, or a government designation. I needed a soldering iron, a CAD workstation, and the conviction that if something can be built, it should be built.
“As you become an adult, you realize that things around you weren't just always there; people made them happen. But only recently have I started to internalize how much tenacity everything requires. That hotel, that park, that railway. The world is a museum of passion projects.”
— John Collison, co-founder of Stripe
The Firefly is one of those things. It did not always exist. Somebody had to make it happen. Here is the part that the researchers may find difficult to hear: I had no idea any of them existed when I started building. I did not read the ambulance desert literature and decide to act. I was an engineer trying to solve a problem nobody else seemed interested in solving — why does no house number on earth signal to a first responder during an emergency? I built the Firefly. And then one day I stumbled on the Vox documentary and discovered that an entire academic ecosystem had spent decades documenting the very crisis my product was already addressing. They had the data. I had the device. They mapped the desert. I had already brought water — I just didn't know the desert had a name yet.
The research is credited throughout this page because it deserves credit. What it does not deserve is the pretense that documentation alone constitutes progress. Men move mankind forward — not organizations, not committees, and not peer-reviewed papers. Often at the expense of their own comfort. The ambulance desert exists. So does the Firefly. One of them saves lives.
Vox produced one of the most compelling documentaries on the ambulance desert crisis, featuring Dr. Yvonne Jonk and bringing the data to a mainstream audience. It is excellent journalism. Watch it. Understand the scope of the problem. Then ask yourself: after watching, do you know what to do about it?
Vox, 2024. “Why millions of Americans can't get an ambulance.” Featuring Yvonne Jonk, PhD.
PBS NewsHour, CBS News, and Governing Magazine have all published substantial coverage. The PBS segment features Nick Nudell, President of the American Paramedic Association, who notes that “elected officials are kicking the can down the road and not owning the funding problem.” The CBS investigation documented Grena Prude's death in Pickens County. Governing published Raphael Barishansky's five-point policy framework. All of it is well-researched. All of it recommends that someone, somewhere, do something.

Gaurav Batta — Founder, Glomensio · Sole Inventor, Firefly · EB-1A Recipient
I was not consulted for any of these productions.
I did reach out — to the Vox team and to Dr. Jonk directly — and they chose not to respond.
Nobody was obligated to, and the world does not revolve around me. But it is worth examining what the experts chose to do instead: they assembled panels of other experts, cited each other's papers, produced a documentary, and then went home. That is their model of expertise — a closed loop of credentialed people admiring the same problem from increasingly sophisticated angles while nothing changes on the ground.
They are professional problem admirers.
I do not need their attention, their approval, or a seat at their table. The Firefly was not built to impress a panel. It was built so a paramedic arriving on a dark street at 2 AM would see the house they were looking for.
But this page exists, in part, as a permanent record that expertise does not always look the way institutions imagine it does. It does not always hold a PhD. It does not always publish in journals. Sometimes it holds a soldering iron and ships a product that works while the credentialed world is still debating whether the problem is adequately defined.
If anyone ever again assembles a conversation about ambulance deserts and emergency visibility without including the only person who engineered a deployed solution — that will say more about their definition of expertise than it does about mine.
The Firefly is not a recommendation. It is not a framework. It is not a pilot program waiting for appropriations. It is a device that ships to your door, mounts to your house, and makes you visible to the people trying to save your life. That is the difference between describing the desert and bringing water.
Every claim on this page is cited. Unlike a white paper, this page also contains something you can buy — and solve the problem.
The landmark chartbook that defined “ambulance desert” and mapped 4.5 million affected Americans across 41 states. Foundational to this entire discussion.
View Publication →Established that running a minimum-access rural ambulance station costs $1.04M/year (2023 dollars). Low-volume agencies face $41,500 per response.
Rural Health Research Gateway →Ongoing research using CDC WONDER data to assess whether living in an ambulance desert is associated with higher mortality rates. Anticipated completion December 2025.
Identified 17 EMS performance measures for rural communities. Valuable framework. Zero of the 17 measures involve deployed technology or products.
PubMed →Federal advisory committee report on EMS access gaps in rural America. Recommends designating EMS as essential service with dedicated public funding.
HRSA Report (PDF) →Substantive investigative journalism documenting the ambulance desert crisis. PBS featured Nick Nudell (American Paramedic Association). CBS documented the Pickens County death. Vox featured Dr. Jonk.
Vox → PBS → CBS → Governing →UVM's NeRHRC contextualizes the ambulance desert crisis and Dr. Jonk's ongoing research into mortality risks associated with living in ambulance deserts.
UVM →AMA's ethics journal examines the structural failures in EMS funding and proposes frameworks for sustainable rural health infrastructure.
AMA Journal of Ethics →While researchers study ambulance deserts from university offices, fire departments and EMS agencies across America have been publishing the same plea for decades: make your house numbers visible. These are not theoretical recommendations. They come from the people who drive the ambulances.
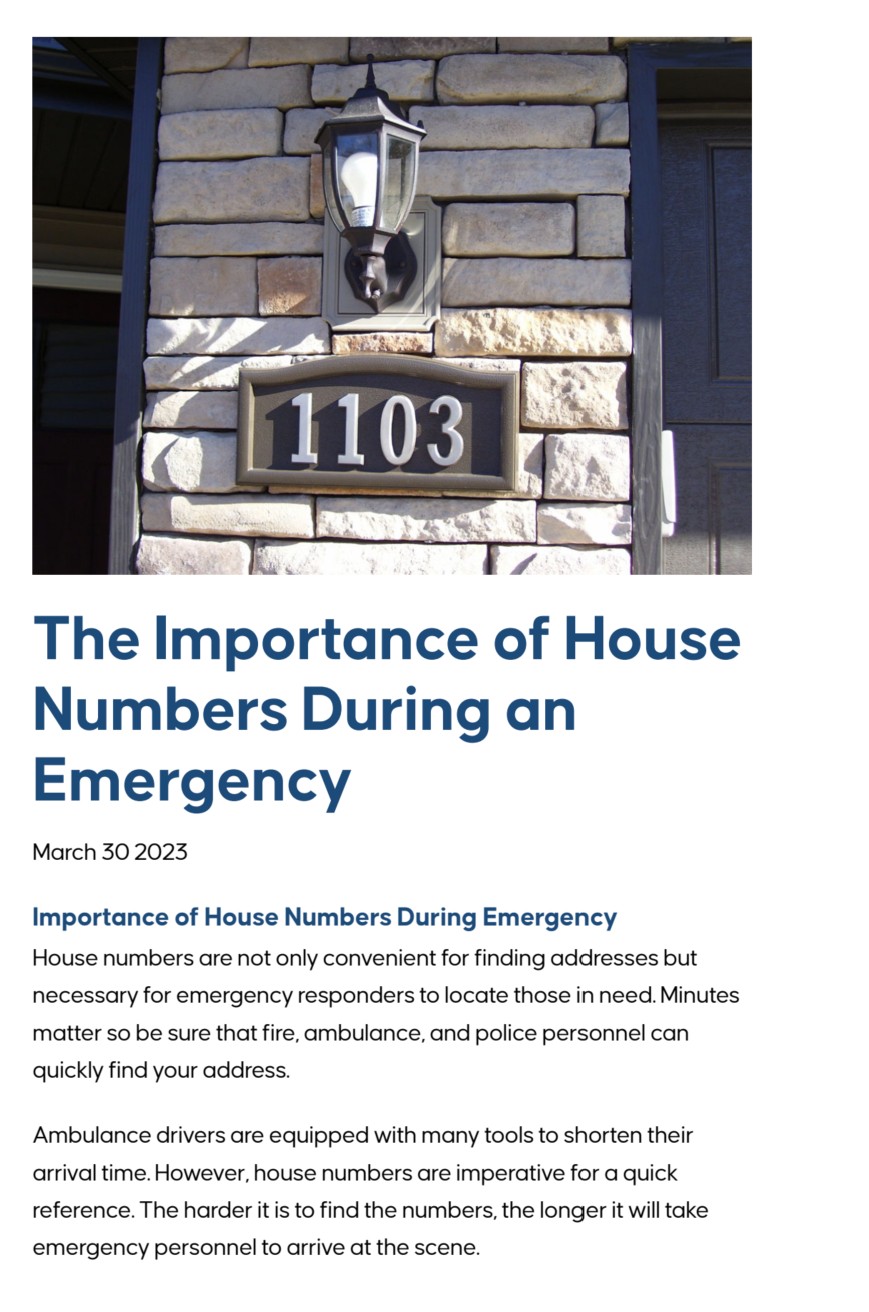
“Unmarked houses cause unnecessary delays... Numbers on a mailbox or post at the end of your driveway should be reflective or white and on a contrasting background.”
“It is very frustrating to responders in the middle of the night responding to your emergency call when we cannot see your address, and we know seconds count.”
“Every second counts when responding to an emergency call, and time spent trying to find your home is time wasted.”
“Firefighters, EMS responders and police officers cannot provide emergency services to you or your family if we cannot find your house.”
The Firefly was built to answer every one of these pleas. Reflective numbers that are visible from both directions? The Firefly is backlit and visible from 1,000+ feet. Illuminated at night? Hardwired LED, always on. Not blocked by bushes? The SOS beacon is visible over and through any obstruction at emergency intensity. The fire departments asked for better house numbers. I built the best one that has ever existed.
The Glomensio Firefly is the only illuminated house number engineered to reduce emergency response time. It does not require a policy change, a funding bill, or a committee recommendation. It requires a screwdriver and 15 minutes.
Safety. Not Surveillance. · Your Home's First Responder.